
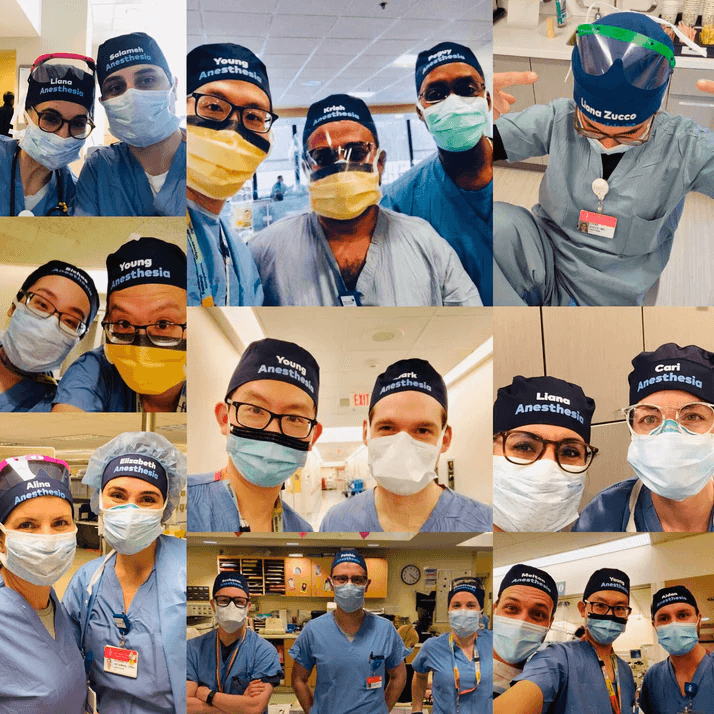
#TheatreCapChallenge - where's the evidence?

TheatreCapChallenge - where's the evidence?
We’ve put some quick links together at the start of this post:
General communication errors
70% of adverse events related to communication errors
Staff misidentification
Numerous cases of adversity including death from wrong blood transfusion.
4 out of 5 female doctors report being misidentified
Increased staff engagement through knowing names
Hearing one’s own name has unique brain functioning activation
A person’s name, to that person, is the sweetest and most important sound in any language.
Staff poor at introductions
How good are doctors at introducing themselves?
Poor compliance with name and role introduction part of Surgical safety checklist
Difficulty for staff to recall names
Social stress-induced cortisol elevation acutely impairs social memory in humans.
Humans poor at remembering names good at remembering faces
Surgeons only knew 44% of names
BJA – name recall worst in Emergency theatres
Studies indicating benefit in using names for communication
Supportive policy
NSW Policy 2008 – Nurse in charge will ensure all staff are easily identifiable
Why use a theatre cap and not just use a badge, lanyard, whiteboard?
Despite policies staff displaying their name and role in theatre is not common
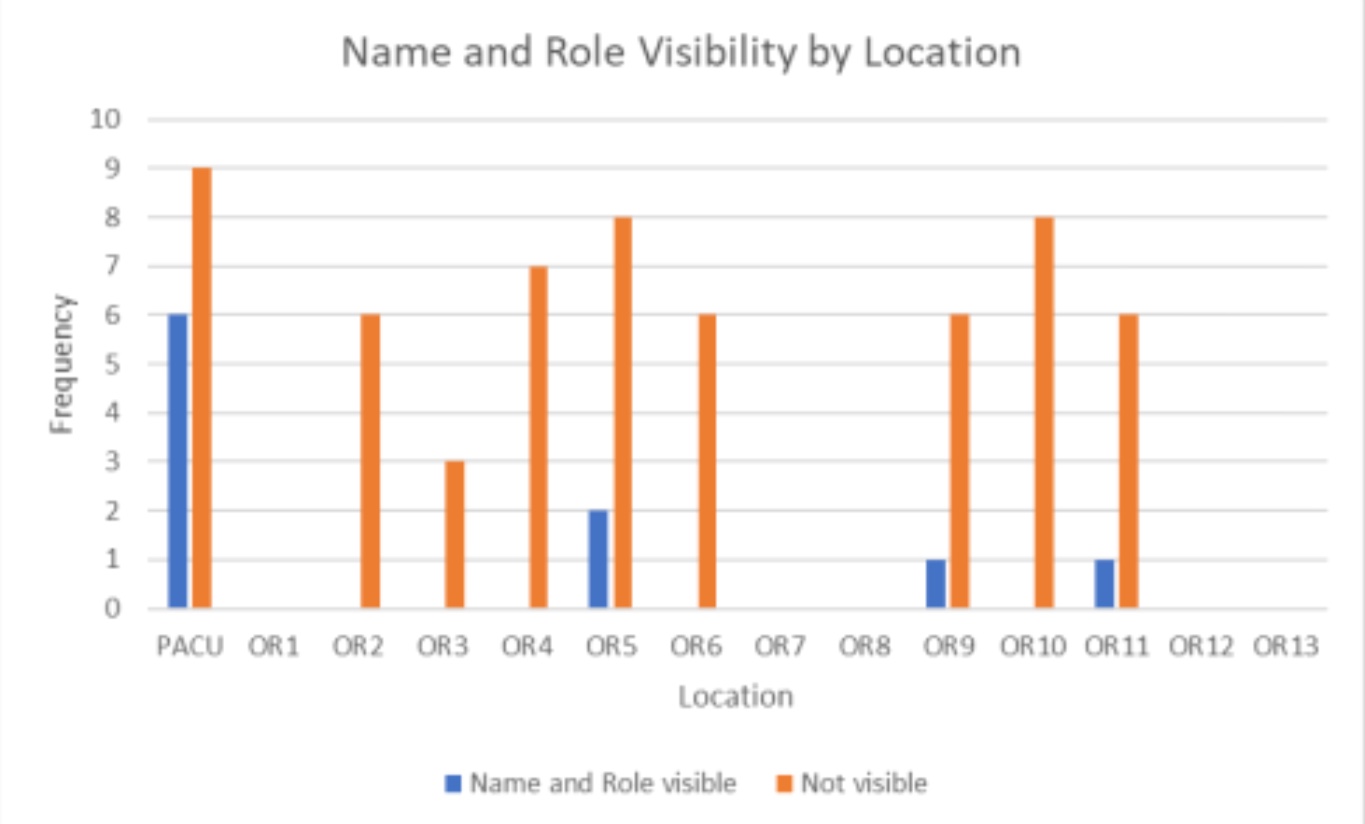
Survey data
Overwhelming support from staff – Imperial College London
Overwhelming support from patients – Queen Elizabeth Hospital
86.5% support on social media survey
Qualitative data suggests introductions help with identification of roles, improve morale and team performance (and see here). However emerging data indicate these introductions have little impact on name recall amongst staff.

Simulation data
Awaiting publication of data from Marlies Schivjen – Professor of Surgery, Amsterdam
Grant from ACI – working group progressing on obtaining outline & data
Support from associations
Endorsed by Australian Society of Anaesthetists
Endorsed by American Association of Surgical Physician Assistants
Australia and New Zealand College of Anaesthetists Bulletin
Support from the European Society of Anaesthesiology and the American Society of Anesthetisology
where's the evidence
Infection Control
Haskins IN, et al. Hernia. 2017.‘There is no association between the type of surgical hat worn and the incidence of postoperative wound events.’
Hussain S, et al. Neurosurgery, Volume 82, Issue 4, 1 April 2018, Pages 548–554.‘Mandatory Change From Surgical Skull Caps to Bouffant Caps Among Operating Room Personnel Does Not Reduce Surgical Site Infections in Class I Surgical Cases.’
Markel T et al, Journal of the American College of Surgeons. October 2017. Volume 225, Issue 4, Supplement 2, Pages e29–e30‘When compared to cloth skull caps, disposable bouffants had greater permeability, greater particulate contamination, and greater passive microbial shed.’
Kothari SN, et al. Journal of the American College of Surgeons. 2018.‘Attending surgeon preference for bouffant vs skull cap does not significantly impact SSI rates after accounting for surgical procedure type.’
Elmously et al. Journal of the American College of Surgeons. 2018.Implementation of the AORN guidelines has not decreased SSIs and has increased healthcare costs.
Policy review
ACORN standards reference Australian Standards which don’t actually relate to headwear.
Excellent review of ACORN Standards as they relate to theatre caps by Dr Rhys Thomas
Environmental Benefit
From ANZCA PS64 (Statement on Environmental Sustainability in Anaesthesia):Use of reusable surgical gowns, dedicated operating theatre footwear and freshly laundered lint free hats will reduce the amount of single use gowns, caps and overshoes that are discarded and add to waste.
Financial benefit
‘I looked at the number of hats that were purchased over a 12 month period. This came to >93,000 hats per year at a cost of NZ$14,600 (AUD 13,410). We have 15 theatres and 430 staff members (includes all surgeons / anaesthetists and surg/anaes registrars).’ – Broadbent J.
Mainstream media support
BBC World News 4.2million likes
Covered by mainstream media throughout the world
If you would like to purchase name and role personalised TheatreCaps please check out our website TheatreCaps.com. All profits from the sale of our caps go towards supporting other patient safety initiatives.
where's the evidence?

{kind=link}
{kind=link}